Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.
Be yourself; Everyone else is already taken.
— Oscar Wilde.
This is the first post on my new blog. I’m just getting this new blog going, so stay tuned for more. Subscribe below to get notified when I post new updates.

When Shruthi* (Names changed to ensure anonymity) walked into my OPD, i could see she longed to have another baby. She lost her five year old last year, in a tragic accident. It didn’t help that she was nearing 40, and time isn’t the kindest to us women. Her previous pregnancy, completely uneventful, did nothing to prepare her for her troubling journey post-partum. Constant anxiety about a baby born a little too early, breast milk that just wouldn’t come in, a thousand customs and opinions forced onto her all culminated in severe depression. She pushed it away, until she found herself contemplating flinging herself and her baby off her fourth floor balcony. That was her wake up call, and she got the professional and emotional help she needed.
She could not (and her family would not let her) risk going through that again.
On the other end of the spectrum is Drishya. Excited and completely giddy with joy when she left the hospital with her firstborn, I was surprised to get a call from her frantic husband two days later. He had left Drishya and the baby alone for all of fifteen minutes for a quick store run, and come home to find a crabby baby and a completely inconsolable wife. After a few conversations and a few days had passed, Drishya was back to her normal self, albeit a little more sleep deprived than usual.
Shruti was ultimately diagnosed with severe post partum depression, while Drishya had a mild case of the baby blues. Either one of these conditions is Not a character flaw, neither are they a result of innate weakness. They are, as the Mayo clinic beautifully puts it, complications of giving birth. The whole process of making a little human, pushing them out into the world and caring for them is not easy. It isn’t meant to be. The process wreaks havoc on a woman’s biology, and messes up her hormones. The brain undergoes structural remodelling, changes that last upto 2 years post delivery. Some scientists believe this eases the transition to motherhood. All this can leave a new mum vulnerable, and tip some women into the abyss.
Experts have recognised the role other factors play in a new mum’s mental health – sociocultural factors, economical conditions, and relationship conflicts. Interestingly enough, a study showed that these factors may play an even bigger role than biology. A few examples from my practice – the woman who cried in disbelief when her fourth girl was born, sure to be immediately evicted from her home. The woman whose in-laws refused to let her formula feed, despite her milk being woefully inadequate. The woman whose marriage fell apart due to infidelity a few days after her baby was born.
Dr. Joraisa DaCosta, a practising psychiatrist, gives us her take. “Motherhood is often represented in an unrealistic and idealised manner on social media, in magazines or even as myths passed on by well meaning family members,” she says. “These myths can put enormous pressure on new mothers and can result in feelings of inadequacy and failure. It is helpful to remember that these myths are often very different from reality.”
Mental health experts divide post-partum issues into three major categories: Baby blues, post partum depression and post partum psychosis.
Baby blues
60 – 80% of mothers will experience the baby blues. It begins about 3 – 5 days after delivery and is distinguished by sudden mood swings, unexplained weeping, irritability, impatience, lack of sleep, crying spells, anxiety, loneliness and a feeling of vulnerability. It subsides without need for medication. Continuous support and education are all that are needed for the mom to bounce back. It is imperative to ensure that moms with baby blues are on the road to recovery. This is because 20% of them progress to a severe form of depression, PPD.
Post partum depression (PPD)
PPD typically appears within 4 – 6 weeks, but may takes months to appear. Women with PPD might not confide in anyone, and family members play an important role identifying it. Symptoms may mimic those of baby blues – in a much more severe form, preventing the woman from even completing daily simple life tasks. She may completely lose interest in food, feel lethargic and teary all the time. Many start to neglect their newborn, with irrational thoughts of harming the little one. Suicidal thoughts may start to take over. These women need psychiatric evaluation and treatment.
Post partum psychosis
This is a severe form of psychiatric illness, where a woman can completely lose touch with reality. She may suffer from auditory or visual hallucinations and behave in an irrational manner. It is imperative to get these women urgent psychiatric help.
Jenny looked at the little wriggling thing being presented to her. Who is this little person? What do I do with her? The nurse put her to Jenny’s breast. As she struggled to feed the bawling thing, the nurse snapped, “What are you doing?? You’re the Mother. Comfort her!”
All through pregnancy, people fawn over you. They tell you you’re glowing, try to guess the sex of your kid, give you their take on delivery. Nobody prepares you for the sheer ugliness of the post partum. In any other situation, going through a major procedure- with a raw wound and heavy bleeding merits you some kind of rest. In this case not only is sleep a luxury, but the entire responsibility of this tiny little being is thrust upon you. The sheer loneliness is overwhelming. Where despite being surrounded by a million people, you are the only one who can feed this child, who is expected to comfort it.
People (most of whom aren’t mothers) seem to believe that motherhood is innate. Every woman Must have the motherly instinct, and those who give birth must automatically know what to do. And some women do. Unfortunately, many others (like Jenny) will tell you that they had to learn – learn to breastfeed, how to get he baby to latch correctly, how to change a diaper, how to hold their baby, how to comfort it. A few sleepless nights; cracked, bleeding nipples and many many frustrated tears later – it becomes second nature.
They say it takes a village to raise a child – and it really does. A village of kindness, a village of understanding. Someone to advise and not domineer, another to cajole without judgement; someone to say, hey. You’re doing a great job. That helplessness you feel – I felt it too – and trust me. It goes away.
Before i say goodbye, here are a couple of do’s and don’t’s to help moms prevent or battle the baby blues, taken from NHS guidance.
Do’s
Do make sure you have treatment for depression in pregnancy. Remember that anxiety may start right in the antenatal period, and do seek the help you need. This is what your doctor is for. Try to be open and honest about your feelings.
Do disclose any past history of depression or mental health problems to your doctor. This helps pick up signs of early depression better.
Do take some time for yourself. Motherhood can be one giant guilt trip, and there is absolutely no harm in taking a little time each day, just to recharge yourself. Leave dad in charge and take a walk on the beach, a run to the grocery store, even a little drive.
Do rest and sleep whenever you can. Ask your partner to night feed at least once so you get a few solid hours of sleep. If you are uncomfortable with formula, you can express breast milk and store it.
Do learn as much as you can about the postpartum while pregnant. Pepper your doctor or new-mom friends with questions. Be informed, and be firm in the choices you make for yourself and your baby. Choose the customs you want to follow and say a firm no if you are uncomfortable with others.
Do find someone you can talk to. Other new moms are usually a great source of comfort. Try to get in some alone time with just you and your partner.
Do eat regularly and healthy, even if you don’t feel up to it. Make time to exercise.
Donts
Don’t blame yourself, your partner or your close relatives. Remember everyone is stressed out and just trying to help. Life is hard right now and irritability and tiredness can lead to arguments. Try to sit down and talk out issues so that your relationship isn’t weak where it needs to be the strongest.
Dont be frightened by your diagnosis. Most women with PPD will get better without medication in 3 – 6 months. Your family may be more understanding if they are aware of the diagnosis.
Don’t hide or ignore the symptoms. Remember, the faster you get help, the faster you will recover. 1 in 4 mothers with PND are still depressed when their child is 1 year old. This is agonising, ruining the joy of new motherhood. It may strain relationships with your partner and render you incapable of taking care of your baby. The longer it lasts, the more likely your baby is to end up with developmental and behavioural issues.
Don’t stop antidepressant medication in pregnancy/ post partum without medical advice.
In the end what pulled Drishya from her funk was her realising she didn’t need to be superwoman. She leaned on her mum a bit more, had regular conversations with me (her doctor), found a great new group of mommy friends, made a little time for herself and her husband. She fell in love with her baby, her new body, her husband all over again. And the whole terrible, beautiful, tiring, wonderful package that is Motherhood.
As we sign off, remember in the words of Albus Dumbledore: Help is Always given to those who ask for it.

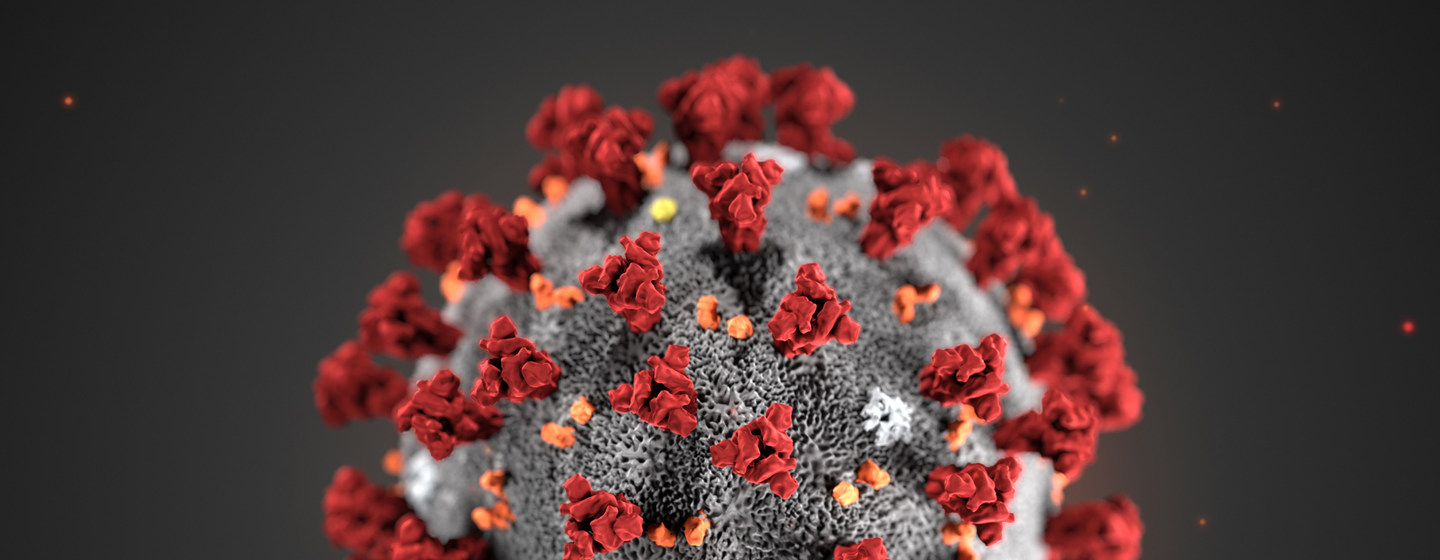
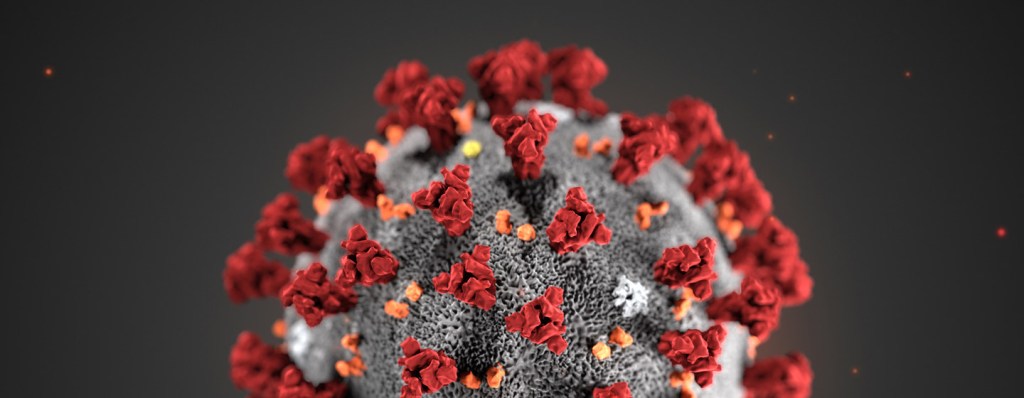
What is COVID-19?
This novel virus is a new strain of the coronavirus, first detected in the city of Wuhan in China. Other Coronavirus infections include the common cold and SARS- CoV (Severe Acute Respiratory Virus).
How bad is it?
As of March 3rd, COVID-19 has killed over 3,100 people and infected over 90,000 people globally. In India, the total number of positive cases touched 46 on Monday, March 9th2020. There are no confirmed cases in Goa as of now.
What are the symptoms?
There are three main symptoms – fever, cough and shortness of breath. These arise about 2 – 14 days after exposure.
What can I do?
According to the Indian Government travel advisory issued March 2020, Indian citizens are advised to refrain from travel to China, Iran, Republic of Korea, Italy and Japan and advised to avoid non-essential travel to other COVID-19 affected countries.
Face -masks have been shown to confer a five-fold increase in protection versus no barrier alone. However, it doesn’t completely obviate the risk. This is because the virus can also spread through tiny aerosols through the eyes, and via fomites (objects or materials which are likely to carry infection, such as clothes, utensils, and furniture.). Wearing a mask when in close contact with a patient of Covid-19 does confer some protection, and people like health care workers or relatives caring for victims are greatly benefitted. however, buying stocks of masks and wearing it in day to day life is not of much use.
The aforementioned ‘fomites’ could be anything! Touching these surfaces that may contain the virus and then subconsciously transferring those germs to your face could risk infection. The key is to avoid touching your face as much as possible. Easier said than done, but a conscious effort goes far.
Wash your hands frequently and well, for at least 20 seconds, preferably with soap and water. Below the blog is a picture of the proper way to wash your hands, initially published by the WHO.
Maintain at least a metre (3 feet) distance between yourself and anyone who is coughing/ sneezing. Crowds are best avoided.
Always sneeze/ cough into a tissue/ handkerchief, your hands or elbow. Dispose of the tissue properly.
If you/ your child are unwell with flu-like symptoms, please stay home from work/ school. If fever/ cough/ cold are accompanied by any sort of trouble breathing, see your doctor as soon as possible.
WHO recommends thoroughly cooking meat and eggs as part of preventing COVID-19.
Who is at risk for a severe infection?
People of any age with severe underlying conditions (heart, lung disease, diabetes, etc.) are at higher risk. Older adults (above 60) are also at higher risk. Children and pregnant women are labelled as ‘at special risk.’ However, most COVID-19 infections in China have been reported in adults. Children and women have been found to be less likely to die from complications of COVID-19 than men.
Pregnancy and the Coronavirus
Are pregnant women at higher risk?
Pregnant women, by virtue of the normal immunological physiological changes of pregnancy are more susceptible to infections. According to the latest research published by the RCOG (British medical authority on pregnancy), pregnant women do not appear to be more prone to the complications of COVID -19. However, the CDC (the Centre for Disease Control and Prevention, America), has placed pregnant women in a group labelled ‘at special risk.’ Thus caution would be wise.
Pregnant women who have a co-existing medical illness are uniquely susceptible.
Can the virus be transmitted to the unborn baby?
Most studies have refuted the claim that the virus can be passed on while the unborn baby is still in utero. However, once the baby is born, it is at risk of infection from droplet infection. The risk of a miscarriage is not increased. Being infected with the COVID-19 does not seem to increase the risk of the baby being born with defects (Coronavirus in Pregnancy, RCOG 9/03/2020).
Finally, in the words of the WHO:

History has see-sawed in its treatment of breastfeeding.
Breast milk has always had a spiritual essence to it. The ancient times held breastfeeding as a matter of great reverence. The Greek goddess Hera’s breastmilk was thought to confer immortality to those who drank it. So much so, that the infant god Hercules was smuggled onto a sleeping Hera’s breast to drink of this liquid gold. When she realised this and pulled away, the spray of her milk into the sky is said to have culminated in the birth of the Milky Way.
A little down the road, the men of yore began to loathe the effect breastfeeding had on the ‘maidenly bosoms’ of their partners. The link to breastmilk and reduced fertility was also recognised, leading those men wanting multiple heirs to despise breastfeeding. The maternal attention to the baby also seemed to lead womens interest away from sex with their partners. All this lead to the insurgence of arguably one of the worse fads in history: The wet nurse.
If men could feel so terribly about breastfeeding, what about women?
Your milk is not enough, you’re starving our child for your own ego. You’re making our child unnecessarily dependent on you, what will we do when you go back to work? You’re feeding too often. You’re feeding too infrequently. You should top up with formula. Your should Never use formula. Your breasts are so unattractive.
This is what a new mother really hears – I am unattractive. I am not a capable mother. I am a terrible wife. I am harming my child.
A recent study has shown that women who have a bad experience breastfeeding, especially in the early post natal period are at higher risk of depression (Watkins et al, 2011). On the other hand, a positive breastfeeding experience can actually be protective against depression.
Pain, anxiety, guilt, reduced milk production. A vicious cycle. One that can be broken.
As doctors, it is our duty to check for depression whenever a mother comes to us with breastfeeding struggles. As family, it is even more important that we help prevent it.
The one thing most of my patients valued the most whilst struggling with breastfeeding is someone who understood. And that meant so much more when that someone was their husband/partner. Have an open discussion about your partners fears, anxieties and tribulations. Give her a pillow to support her back when she’s breastfeeding. Pour her a glass of water (breastfeeding makes her thirsty!). Offer to burp the baby when she’s done. Breast feeding cravings are real! Take her out to eat once in a while. Little things help her know she is not in this alone.
Stay away from negative vibes. Even if its a dear relative, if someone is making your wife feel small for her breastfeeding practices- notice, validate her feelings and stand by her.
To really be supportive, husbands and wives need to be on the same page. Make sure you find out all you can about breastfeeding Before the baby comes. Any questions daddy has as well, ask your doctor. Go in to appointments as a couple and come up with a solid breastfeeding strategy.
Husbands, know that breastfeeding is not just a sit down, easy, do nothing job for mamas. Yes, it can be wonderful. But it is also a draining, exhausting exercise, one she has to repeat every two hours, for about 20 minutes at a time for months on end. Studies have shown that breastfeeding sucks so much calcium out of a mother, it can cause her to lose 3 – 5% of her bone mass in one year.
So to take care of baby, take care of that mama. Diet, nutrition, posture, exercise, mental well being, alone time – these are all equally important. A happy mama translates to a happy baby.
Fortunately, as time passed it suddenly became fashionable again to feed your own baby, and wet nurses fell out of favour. Aristocratic women in Europe even boasted about breastfeeding their own children!
And so we come full circle. Remember, the decision and resolve to breastfeed is really personal. The manner in which you do its equally personal. You don’t owe anyone any explanations. Anyone that is, except your baby, your partner and yourself.
The author is an Obstetrician -Gynaecologist practicing in Dr. Antonio Pinto do Rosario Hospital in Porvorim Goa, and a mother of two, who has had (at best) a rocky relationship with breastfeeding.
Just off 14 hours of labour- exhausted, excited, longing for some rest, hungry as heck – thats just your baby. Mama is emotionally and physically pretty much drained as well. So how do we do this feeding thing? This is your guide to navigating your hospital stay while breastfeeding your baby.
Long before you even start thinking about feeding, your breasts are already preparing for your baby. Come late first trimester and they’ve already begun to enlarge, the milk ducts and milk secreting cells developing. Your body will do all the work for you. The only thing one needs to watch out for are the contour of ones nipples. Some women have a ‘flat’ or ‘inverted’ nipple – both make it difficult for baby to latch properly. Ask your doctor to rule these out before delivery. These conditions are treated by easing the nipple out using negative pressure – a ‘nipple puller’ or a syringe with one end cut off will do the trick. Even a breast pump can help. You can start this antenatally, and continue doing it just before feeds when the baby arrives.
Forget birth partner, you need a breast feeding partner! No-one tells you that you might have an episiotomy, or even a caesarean. Both make holding your baby in those first few hours difficult. When Diya came, I needed someone to hold her to the breast every two hours, I couldn’t do it on my own. The hospital nurses were not always free to do this, so having someone with me who was experienced with holding babies (those wobbly necks!) was really helpful. I also couldn’t get out of bed to change her nappies, pick her up or comfort her. So find that superstar and recruit them before you get to hospital.
2. Sleepy baby!
Ali was born 4 weeks early. She just wouldn’t latch, wouldn’t feed, would do nothing but sleep! I was intent on exclusively breastfeeding her. Some of the methods the midwives tried were tickling her feet, and scratching her behind her ears, rather like you would do to a cat, all in the effort of waking her up. When she crossed the five hour mark without a feed, the head nurse put her foot down and gave her a little expressed milk via paladai (a tiny vessel with a long snout used for feeding babies). Premature babies might not have such a strong suckle reflex as a fully mature baby, and may need help feeding (More on feeding premature babies in an upcoming post).
Ali soon caught up, and was feeding like a champ in a few days. Theres no shame in resorting to paladai, sometimes even formula if the occasion absolutely calls for it. Remember, breast is best, but if it’s not happening despite your best efforts, ultimately a baby must be fed. Breastfeeding does not, and should not define you as a mother.
3. Making sure babys full and happy.
The problem with breast feeding is that it doesn’t give you a visual of the quantity of milk your baby is getting. So how do we make sure babys getting enough?
– Listen to your body. When your baby starts to suck, the combination of the suckling on the nipple and the affection that floods through you releases a hormone prolactin and milk starts to form. You will begin to feel a sensation – rather like pins and needles – in your breasts as they start to fill up. There will be a certain hardness to breasts when they are full, gradually softening as they empty.
-Make sure baby completely empties one breast before moving to the next. This takes about 5 – 10 minutes, but a newborn may suck on one breast for upto 20 minutes. The initial milk that is secreted, the fore-milk, is watery and only satisfies babys thirst. The hind-milk is full of the energy that baby needs to satisfy his/ her hunger, and making it imperative that baby empties Both breasts completely during each feed.
-Listen. You may be able to hear baby swallowing, this is a good sign that milk production is adequate.
-Your baby should put out enough urine. With cloth diapers, this entails 6 – 8 diapers per day, sometimes more. If you use store bought pampers, this entails at least 2 full, heavy nappies per day in the first 48 hours. By five days this should be at least 5 – 6 heavy, wet nappies per day. By the end of two weeks, baby poo should turn a mustard colour and there should be at least two episodes of poo per 24 hours. Breast fed babies actually poop more than formula fed babies, and this is normal. As long as the poop isnt too watery, and baby is putting out enough urine, there is no need to worry.
Side Note: Your baby may poop as soon as you start feeds. This is normal, and known as the ‘gastro- colic reflex.’ Gastro = stomach, colon = large intestine.
-Weight gain. Most babies actually lose weight (7 – 10% of birthweight) in the first few days. They regain their birth weight by 10 – 14 days and then steadily gain weight.
-Baby should be happy, sleepy and content after a feed. A baby that’s irritable, crying too much or not sleeping well might either not be getting enough milk, or may be colicky. Its best to consult your doctor to establish why.
4. The diet.
The hospital isn’t the best place to get a great diet. Breast milk may be a little slow to come to some women, taking a few days to really come in. How can you improve your flow?
Some patients, especially post caesarean may not be able to be on a full diet. Don’t worry, as this is usually only for one or two days, and very necessary for you to recover from such a major surgery. The doctor will sign off on your diet soon enough, and once you start eating well, the milk will begin to flow.
Hydrate, hydrate, hydrate. Drink fluids like you’ve been lost in the Sahara for the past 9 months. At least 3 litres of fluid per day, and if a good part of that can be milk, milkshakes, lassi, curd, yoghurt; even better.
Eat whatever you feel like eating. As long as it’s not raw, spicy, shellfish or prone to give you diarrhoea, just eat. Forget pregnancy cravings, breastfeeding cravings are a whole different ballgame. I just had a patient complain that her kin was too busy making sure she was eating healthy to tend to her cravings! As someone who had a friend bake an entire date-and-caramel cake, and then proceeded to Devour it on day 5 of my child’s birth, I completely sympathise.
*Disclaimer: Might not have been a great idea to devour an entire cake 5 days after giving birth!
More on a good, healthy (and yummy) breastfeeding diet in an upcoming post.
5. In Sickness and in Health
Sick Mamas, a doctor will usually not prescribe a medication to a new mother that cannot be taken during feeding. If you are on antibiotics for any reason, it is usually safe to continue feeding. There are a few special medications and illnesses that may require you to stop feeding, or express milk and feed your baby. Some of these include an attack of chicken pox just before/ during delivery, some types of tuberculosis, medications taken for some forms of psychiatric illnesses. The relationship with HIV and feeding is complicated. It is best to consult your doctor for individual concerns.
What about a sick baby?
My worst nightmare came true three days after Diya was born. Her poo seemed runny, I had been warned to expect that. But then it kept coming, getting more and more watery with each episode. When we checked, her temperature clocked in at 102 degrees F. We alerted the paediatrician, and he put her straight into the ICU, on IV antibiotics. Feeding her became my sole mission, I was there on the clock, every two hours. Thanks to a great NICU staff who coached and coaxed me through those days, Diya was able to avoid an IV drip. She came out 5 days later, on Christmas Day, well enough to go home.
Sick babies must be fed well, and fed often. The antibodies you give your baby through breast milk are priceless. Feeding every two hours goes a long way in preventing dehydration that might occur through treatments like phototherapy (a kind of light the baby is placed under to get rid of jaundice).
6. Of breast engorgement and cracked nipples.
Cracked, bleeding, painful nipples and swollen breasts? No wonder the Mughals had wet nurses!
If these things are happening to you, chances are the baby is not latching properly. The hospital is the best place to get this sorted. I always make sure I observe the mother feeding her baby first hand, the very best way to gauge if latching is correct. Theres only so much you can convey to your doctor via a conversation.
Still, some ways you can gauge for yourself are
If you do begin to get a cracked nipple or fissure, the best medicine is breast milk. Just apply a little on the nipple after you’re done feeding. Breast engorgement takes you down the slippery and painful road to a breast abscess. Correct latching saves you the trip.
If you’re confident feeding and baby is well within her limits of weight loss (or gaining weight), then your hospital stay can come to a close, and we can sign off till next time.
Until then, here’s wishing you continued happiness and positivity on your journey.
Heres a picture of Diya, our breast-fed Diva, rocking her IV-line while in the ICU, all of 5 days old.

The author is an Obstetrician -Gynaecologist practicing in Dr. Antonio Pinto do Rosario Hospital in Porvorim Goa, and a mother of two, who has had (at best) a rocky relationship with breastfeeding.

The day my baby was born was also the first time someone made me feel like a failure as a mother.
Diya was howling, I was trying to get her to latch. After many futile attempts, both Diya and I were in tears, and nowhere close to latching. A prim nurse marched into my hospital room, snatched my baby from me and soothed her. She turned to me and snapped, “Cant you comfort her? What kind of mother are you?”
Giving birth doesn’t automatically give you all the answers. Most people expect you to instinctively know what to do, and in some ways that is true. But there are so many things I wish I’d known before I began my journey.
The first day. WHO recommends three solid strategies to help initiate and sustain breastfeeding.
Other interesting and must know facts for day one.
Your baby’s stomach is the size of a cherry on the first day of life! That means whatever milk you produce is more than enough for your little one. Water, formula are best avoided.
Colostrum. Otherwise known as liquid gold. This is the name given to the milk produced on the first day. No formula, no matter how expensive is going to be able to provide your baby with the heady little cocktail of nutrition, antibodies, protein and fat that colostrum provides. The quantity produced may not seem like much, but proteins and fat are so highly concentrated it is more than enough to satisfy your baby. The composition is such that your newborns fragile, developing intestinal system is not harmed and able to digest well. Colostrum also encourages baby to have their first major poop, getting rid of ‘Meconium'(the green coloured substance present in baby intestines at birth) and preventing certain kinds of jaundice.
Your baby is learning to breastfeed. And so are you! Dont put too much pressure on yourself or your baby. Learn to respond to his/ her cues. Not latching? Ask yourself if there could be another reason. Are they gassy? Do they have a wet diaper? Try other avenues – burp them, change their diaper, comfort them. Try again. You and your baby have to find your own rhythm. It is never one size that fits all. And once you fall into it, all will be well.
Your baby has innate reflexes that will enable him/ her to feed. Never push the nipple directly into the mouth, rather graze the angle of her lips with your breast. The baby instinctively turns and opens their mouth, searching for the nipple and latching on. Make sure the Entire nipple is in the babys mouth. This includes the wide area of pigmented skin around the nipple elevation. This will ensure the baby uses his/ her tongue to suck, and not those (surprisingly) hard little gums – which is the cause of most cracks, fissures and painful feeding.
Four years and two breast fed babies down the line, I hear a baby fussing through the door of one of my patients rooms. Peeping in, I see a young mother intent on getting her baby to latch. The little one isn’t having it, yelling her little lungs out. I put my hand on her shoulder, a mark of solidarity. “Soothe her. Then try feeding her again.” Mama looks up and me and wordlessly changes tactics. A couple of cuddles, coos and I-Love-Yous later, mama and baby were latched and feeding well.
Good luck moms. Heres wishing you a satisfying, beautiful start to a beautiful journey.
The first six months of my baby’s life, I didn’t use a car seat.
I had heard of car seats, read the recommendations, done the homework. I even bought one and installed it. It seemed a bit ‘Fancy.’ The distances we travelled were always really short. And everyone else had an opinion – her howling was ‘unnecessary.’ I was ‘making my child cry.’ She’d be more comfortable in a lap.
Even my best friend, a mother of two boys, yelling at me didn’t help. I laughed her admonitions off with all the confidence of a young, inexperienced first time mum.
It took one sharp brake and my baby flying out of my arms, almost falling over the gear-box for me to finally realise I was putting my child at risk. I started keeping my baby firmly strapped in – no matter what.
The statistics are terrifying. In the ten minutes you will take to read this article, two people in India will have lost their lives to road traffic accidents. Thats one person dying every 3.6 minutes. In Goa, there were 3,917 accidents in 2017 (Road Accidents in India (2017) report), killing 328 people and leaving 1,922 injured.
Children are particularly at risk. Infants have soft spinal cords, and can have serious head, neck and spine injuries. Children can be thrown through windshields, against seats resulting in horrific injuries. In America, deaths of children from road traffic injuries surpasses those caused collectively by all childhood diseases. More than half these deaths are in children that were unrestrained.
So what can you do to keep your baby safe?
Children less than 13 years are always safer in the back seat of a car, firmly strapped in. When they are less than 5 years old, they are safest in a car seat.
Airbags. Life saving for adults, potentially fatal for kids. Airbags open with great force, >200mph, and were designed for 75 Kg men. They can cause serious head and neck injuries to children. Never, ever put a child in the potential path of an airbag, even if buckled in a car seat.
Do your research. Check out reviews when purchasing a seat, and make sure it comes with a user manual. When buying second hand, do NOT buy a seat older than 6 years or one that has been in a car crash. It is always safer to buy a second hand seat from family/ close friends rather than a stranger.
Buckle your child in safely. Mayo Clinic offers advice on how to make sure your child is snug and secure:
“Buckle the harness straps and chest clip, with the chest clip even with your child’s armpits. Make sure the straps and clip lie flat against your child’s chest and over his or her hips with no slack.
In the rear-facing position, recline the car seat according to the manufacturer’s instructions so that your child’s head doesn’t flop forward. Babies must ride semi-reclined to keep their airways open.Keep in mind that as your child grows, you might need to adjust the angle.“
Beware of flying objects. That favourite toy lying on the backseat? Put it away. It can prove injurious in a crash. The same goes for unrestrained adults. Buckle in, and make sure everyone else does too. Also sets a great example for young kids to pick up safe road habits.
Start early! Baby’s first trip home should be in a car seat. Be wary of kids in car seats that are less than 3-4 months as head control hasn’t kicked in yet. Sit at the back with them to ensure the head is well supported. Small, tightly rolled blankets placed on either side can be used to provide head and neck support if necessary. Special care to be taken that this doesn’t become a suffocation hazard.
Forward or rear facing car seats? The AAP (American Academy of Paediatrics) recommends that kids remain in rear facing car seats until they reach the upper limit of height and weight recommended by the manufacturer. This can extend upto 16 Kgs depending on your car seat model. Age is not a deciding factor, and this can extend upto 3 – 4 years of age.
Lastly, feast your eyes on Zoe snugly buckled in, a proud alum of Pinto Rosario Hospital, car seat enthusiast and our little Ambassador for car safety.
Stay safe. Signing off,
Your friendly neighbourhood ObGyn.

This is an example post, originally published as part of Blogging University. Enroll in one of our ten programs, and start your blog right.
You’re going to publish a post today. Don’t worry about how your blog looks. Don’t worry if you haven’t given it a name yet, or you’re feeling overwhelmed. Just click the “New Post” button, and tell us why you’re here.
Why do this?
The post can be short or long, a personal intro to your life or a bloggy mission statement, a manifesto for the future or a simple outline of your the types of things you hope to publish.
To help you get started, here are a few questions:
You’re not locked into any of this; one of the wonderful things about blogs is how they constantly evolve as we learn, grow, and interact with one another — but it’s good to know where and why you started, and articulating your goals may just give you a few other post ideas.
Can’t think how to get started? Just write the first thing that pops into your head. Anne Lamott, author of a book on writing we love, says that you need to give yourself permission to write a “crappy first draft”. Anne makes a great point — just start writing, and worry about editing it later.
When you’re ready to publish, give your post three to five tags that describe your blog’s focus — writing, photography, fiction, parenting, food, cars, movies, sports, whatever. These tags will help others who care about your topics find you in the Reader. Make sure one of the tags is “zerotohero,” so other new bloggers can find you, too.
